
From the Karolinska Institutet, Department of Clinical Sciences, Danderyd Hospital, Division of Rehabilitation Medicine, Stockholm, Sweden
Objective: To explore the usability and effects of an assistive soft robotic glove in the home setting after stroke or multiple sclerosis.
Design: A mixed methods design.
Methods: Participants with stroke (n = 10) or multiple sclerosis (n = 10) were clinically assessed, and instructed to use the glove in activities of daily living for 6 weeks. They reported their experience of using the glove via weekly telephone interviews and one semi-structured interview.
Results: The soft robotic glove was used by participants in a wide variety of activities of daily living. Perceived beneficial effects while using the glove were a sustained and a strong grip. Disadvantages of using the glove were a lack of assistance in hand opening function and the glove not being usable for fine hand use. The glove was found to be useful by two-thirds of participants who completed the study, mainly by participants with moderate limitations in hand activity and an overall level of functioning that allowed participation in everyday life activities.
Conclusion: This study identified a subgroup of participants, who found the glove useful in activities requiring a strong and prolonged grip but not fine hand use, and highlights aspects for consideration in the further development of soft hand robotics for sustained use in a larger population living with a central nervous system lesion.
Key words: robotics; assistive technology; stroke; multiple sclerosis; evaluation; qualitative; quantitative.
Accepted Jan 16, 2020; Epub ahead of print Jan 29, 2020
J Rehabil Med 2020; 52: jrm00027
Correspondence address: Susanne Palmcrantz, University Department of Rehabilitation Medicine, Danderyd Hospital, Stockholm, SE- 182 88 Sweden. E-mail: susanne.palmcrantz@ki.se
To explore factors impacting on the usability of an assistive soft robotic glove in the home setting after stroke or multiple sclerosis. Twenty participants living with the effects of stroke or multiple sclerosis used the assistive glove in the home for 6 weeks. Perceived usability was reported in weekly telephone interviews and one semi-structured interview. Functioning was clinically assessed. Perceived beneficial effects were a sustained and strong grip. Reported disadvantages were a lack of assistance in opening the hand, lack of wrist support, and the glove not being usable for fine hand use. The glove was found to be useful mainly by participants with moderate limitations in hand activity and an overall level of functioning that allowed participation in everyday life activities. This study identified a subgroup of participants, who found the glove useful in activities requiring a strong and prolonged grip but not for fine hand use, and highlights aspects for consideration in the further development of soft hand robotics for sustained use in a larger population living with a central nervous system lesion.
S
troke and multiple sclerosis (MS) are neurological conditions that commonly cause upper limb impairment, long-term disability and dependence in activities of daily living (ADL) worldwide (1–5).
The annual incidence rate of stroke in Sweden is approximately 300 per 100,000 inhabitants (6) and a majority of stroke survivors experience impaired function in the upper limb and hand (7). Recovery of hand function after stroke is, therefore, crucial and is one of the major goals of rehabilitation. However, only approximately 50% of stroke patients with initial arm paresis regain full function (7). Despite increasing evidence that specific rehabilitation interventions, e.g. constraint-induced movement therapy (CIMT), may improve hand function after stroke (8), many patients are left with impaired hand motor function that limits their everyday activities and restricts participation in work and other social life.
The estimated prevalence of MS in Sweden is 17,500 (4) and upper extremity function is impaired in a majority of patients. Johansson et al. reported difficulties with manual dexterity in up to 79% of 219 patients (5) and Cano et al. reported that 51% out of 285 patients experienced at least moderate impairments in hand function, impacting on activity performance, leaving only 20% who reported no limitations or restrictions (9).
Therefore, there is a need for new, innovative and individually designed interventions to improve function, through restorative treatments or by use of compensatory strategies and assistive devices, in many people with prior stroke or MS. Currently, numerous supportive tools, including various orthoses, are used for static support of, for example, the wrist. New technologies aiming to improve manual activity performance are in various stages of development, but, to date, evidence demonstrating the effects of a device that improves hand motor function in everyday life has been scarce.
During the last decade, various electromechanical and robot-assisted devices for arm and hand training have been developed and tested, although the quality of the evidence regarding potential effects is still limited (10). Most robotic systems are relatively heavy and stiff, but current developers have produced more lightweight and flexible solutions (11–13). One is a new glove, based on Robotic SEM™ Technology (14) (Fig. 1), which offers the possibility of increasing grip strength for patients with impaired hand function. The SEM™ Glove device is designed to be slim, lightweight, neat, comfortable, and is intended to be worn as a glove. The technology concept goes beyond other state-of-the-art devices by introducing an “intention detection” logic that activates support if, and only if, the wearer initiates movement with a natural movement intention. This is achieved by sensors on the fingertips that detect minimal pressure changes initiated by the wearer, which are transferred to actuators. These respond immediately in order to facilitate the intended movement.
Experiences with the SEM Glove in patients with impaired hand function, but some retained extensor function in the fingers, suggest that it may support hand function and increase independence in everyday activities (15; and unpublished data). However, data on the feasibility of the SEM Glove for use by patients with impaired hand function due to central paresis are scarce. Recently, observations were reported on the feasibility of the SEM Glove in a group of 5 patients in the chronic phase after stroke (16), but more data are needed to guide the clinical application and further development of this glove. The primary aim of this study was therefore to determine what factors affect the usability of the assistive SEM Glove when used in the home setting after stroke or MS, in relation to diagnosis, functioning, disability and perceived usability.
Fig. 1. Motor performance with the SEM Glove. The SEM Glove provides actuation for the thumb, middle and ring fingers. The applied force is measured by pressure sensitive sensors at the tip of the fingers of the glove and is regulated by the pull of thin lines that run through a cord and attach to the motors. A case that can be worn at the waist or in a bag includes the motors, computer, batteries and controller (reproduced with permission from Bioservo Technologies Inc).
Study participants
Participants aged 18 years or older with impaired hand function after stroke (n = 10) or MS (n = 10) were recruited from outpatient rehabilitation clinics in Stockholm County, Sweden. Recruitment was administered by the Division of Rehabilitation Medicine at Danderyd Hospital. Study information was distributed to physiotherapists and made available to patients at the clinics. Information was also made available to people with stroke or MS who were visiting exhibitions for assistive devices, including the SEM Glove.
Eligible for inclusion were people with stroke (> 6 months since onset) or MS (stable condition > 6 months) and perceived limitations in ADL due to impaired hand function. A minimum of visible activation of the wrist and finger extensor muscles was required. In addition, participants were required to be able to handle the SEM Glove with or without support from a significant other or a personal assistant.
Exclusion criteria were: severe speech and language or cognitive impairments preventing informed consent or understanding and complying with study instructions; other diseases that might affect hand function; other somatic or psychiatric conditions or drug abuse that may interfere with study participation; ongoing rehabilitation intervention or participation in another clinical study that might have an impact on hand function; and treatment with intramuscular injections of Botulinum toxin within less than 3 months prior to study start
Data collection
A mixed methods design was used (17). Quantitative data were collected before the intervention and qualitative data during and after the intervention. Sociodemographic data included age, sex, current occupation, civil/cohabitant status, time since stroke/time since MS diagnosis. The modified Rankin Scale (mRS) was used to categorize the level of overall functioning and a cut-off for disability was set at mRS > 1 point (where 1 = no significant disability despite symptoms; able to carry out all usual duties and activities) (18, 19); the Barthel Index (BI) (20) was used to assess degree of independence and a cut-off for independence was set at BI ≥ 95 points (21).
Standardized measures of body function of the upper limb included the active range of wrist movement assessed with a goniometer and grip strength by use of a digital hand dynamometer (www.Saehan.com) with a cut-off for impairment set based on adult norms (women < 22 kg right and < 20 kg left and men < 37 kg right and < 35 kg left) (22). Furthermore, somatosensory function (touch and proprioception), passive movement and pain was assessed with the Fugl-Meyer sub-scales (23); spasticity with the Modified Ashworth scale (24), and the neural component of resistance to passive stretch was quantified by use of the NeuroFlexor method (25–27). A neural component > 3.4 Newton (N) was considered as hand spasticity (28). Gross manual dexterity was assessed with the Box and Block Test (BBT), and impairment level was set based on adult norms (women < 66 blocks right and < 64 blocks left and men < 63 blocks right and < 68 blocks left) (29). The ability to move and handle objects was assessed by use of the Action Research Arm Test (ARAT) (30).
Qualitative data for everyday activity performance and perceptions of using the SEM Glove were collected via weekly structured telephone interviews conducted by the same physiotherapist who performed the clinical assessments and fitted the SEM Glove. The interview included questions related to overall use of the SEM Glove and specified activities, as well as advantages and disadvantages experienced when using the glove, including adverse events. At the end of the intervention, participants were asked to report their experiences in a semi-structured interview performed by an experienced therapist not otherwise involved in the study. The interview guide included questions related to perceived usability of the glove in ADL and potential effects on hand function and/or activity.
Intervention procedure
The SEM Glove was fitted on the hand perceived as being impaired by the participant and identified as being impaired by the physiotherapist, based on the initial assessments. The physiotherapist had been trained in this procedure by a specialist from the SEM Glove manufacturer (Bioservo Technologies Inc, Stockholm, Sweden). The fitting included settings for power transferred by the tendons and sensitivity of the sensors for each finger. Moreover, the participant was educated in donning and doffing the glove, changing the batteries, and given written instructions on the functioning of the glove. The participant was instructed to use the glove in ADL, on a daily basis, for a period of 6 weeks.
Ethical approval
The study was approved by the Regional Ethical Review Board in Stockholm (2016/980-31/1).
Data analyses
A mixed methods embedded design was used (17). Descriptive statistics were used for quantitative data. Information regarding activities in which the SEM Glove had been used was grouped according to diagnosis and the International Classification of Functioning, Disability and Health (ICF) (31). The interviews were digitally recorded and transcribed verbatim. Qualitative content analysis was used for analysis (32). The texts were read through carefully, condensed to meaningful units and coded into subcategories and categories. The subcategories and categories were critically examined to secure trustworthiness. To allow analysis of potential differences in perceived usability related to diagnosis, subcategories were labelled with the informants’ diagnoses. To explore how diagnosis and level of functioning and disability were related to perceived usability, quantitative and qualitative data were merged by tabulating the patient’s level of functioning and disability combined with their response to a question posed in the semi-structured interview related to the experienced usability of the glove.
Participants’ characteristics
Characteristics of the included participants (stroke n = 10, MS n = 10) are shown in Table I. Occurrence of activity limitations and impairments in the upper extremity of the gloved hand are shown in Table II. Except for a lower BI score and grip strength among participants with MS, activity limitations and impairments in the upper extremity were in a similar range in the diagnostic groups (Table II). Furthermore, 2 participants in the stroke group and MS group, respectively, could actively extend their wrist, but not above 0° against gravity, and 5 participants in the stroke group and 3 participants in the MS group could not fully extend all fingers against gravity.
Table I. Characteristics of the included participants
Table II. Results of assessments of activity limitations and impairments in the upper extremity of the gloved hand
Experiences of using the SEM Glove in activities of daily living
Participant’s contributions to the study are shown in Fig. 2. Of the 20 included participants, 19 shared their experiences of using the SEM Glove in ADL in weekly telephone interviews during the intervention (Fig. 2). The participants with stroke used the glove for a mean of 4 weeks (standard deviation (SD) 2.1, range 0–6 weeks) as did the participants with MS (mean 4 weeks, SD 1.8, range 2–6 weeks). One participant with stroke never started using the glove in the home setting and was followed up on only one occasion.
Fig. 2. Flow chart of participants’ contribution to the study. MS: multiple sclerosis.
Reasons for not using the SEM Glove for the full 6 weeks among participants in the stroke group were problems with setting the glove, illness, and private circumstances. In the MS group, reported reasons for not using the glove in the home were illness, hospitalization, not finding suitable activities either due to overall disability or the fact that the need for assistance in fine hand use were not met by the glove. Additional reasons were related to the construction of the glove, which was perceived as bulky and unwieldy, or private circumstances.
No adverse events were reported, with the exception of one participant in whom the SEM Glove band used to attach the cord to the forearm scratched the skin. This participant was then instructed to use the glove only with long-sleeved clothing.
Participants’ reported activities chosen to explore the usability of the SEM Glove derived in the weekly telephone interviews are shown in Table III and reported advantages and disadvantages of using the glove in ADL are shown in Table IV.
Table III. Participants’ reported activities chosen to explore the usability of the SEM Glove (multiple sclerosis (MS) n = 9, Stroke n = 10)
Table IV. Participants´ reported beneficial effects and disadvantages of using the SEM glove in activities of daily living (ADL) (multiple sclerosis (MS) n = 9, stroke n = 10)
Fifteen participants (stroke n = 8, MS n = 7) reported their overall experience of using the SEM Glove in semi-structured interviews at the end of the intervention (Fig. 2). The categories that emerged from the interviews were: body function and activity performance in ADL; general activity level in ADL; lasting effects on functioning; level of functioning needed for beneficial effects; learning period; activity performance related to the construction of the glove. Furthermore, 10 participants found the glove to be useful in some ADL and 5 did not. Two groups emerged in terms of their experience of using the glove in ADL. The first group (MS n = 4 and stroke n = 6) included participants who found the glove to be useful in some ADL and the second group (MS n = 3, stroke n = 2) included participants who did not find the glove useful in any ADL. Level of functioning and disability among participants, who found the glove usable in ADL, is shown in Table V, and of participants who did not find the glove usable in Table VI, together with reported aspects of usability. The representation of participants with Stroke and MS is presented in brackets throughout the text.
Table V. Clinical characteristics of the participants who found the glove to be useful in some ADL (n = 10)
Table VI. Clinical characteristics of the participants who did not find the SEM Glove to be useful in ADL (n = 5)
Body function and activity performance in ADL among participants who found the SEM Glove useful in ADL
The SEM Glove enabled participants to produce more power and to hold and sustain the grip (MS and stroke), as well as improving the quality of the grip, which enabled handling and holding household objects (MS and stroke).
“The benefit has been that I have been able to use my left hand to lift things up and grasp things. Well, first grasp and then lift…. couldn’t before.”
Moreover, the SEM Glove was reported to enable the use of the gloved hand as an assistive hand while handling and holding household objects (MS) and to carry objects in one hand while walking with assistive devices (MS and stroke) and pursuing bimanual activities, such as vacuum cleaning, pulling up trousers and using a wheelbarrow (stroke).
“Really, I’m not strong enough to hold anything for at particularly long time… So….but, when I have had the glove, I have been able to hold a pack of butter and carry it to the table and so on… Good for vacuum-cleaning too, two-hand grip”
The SEM Glove was found to be assistive in pursuing leisure activities (MS and stroke) and physical rehabilitation interventions (stroke).
“Yes, and then, so, if I’m sitting in the garage or the tool shed, I can hold a thing much better with the left hand now.”
For other participants the physical training exercises were the only activities in which the SEM Glove was found to be useful (MS, stroke). The glove enabled these participants to produce more power and to hold and sustain the grip during training (MS, stroke).
“No, I didn’t get the hang of it in the way I wanted to….. So, then, I´ve seen it more as a training… device rather than assistance in ADL existence.”
General activity level in ADL among participants who found the SEM Glove useful in ADL
One reflection made by participants who were dependent as regards ADL, was that they performed ADL to a minimal extent and had therefore little use of the SEM Glove (MS, stroke).
“….I have come to realize that the life I live ……there are very few activities that I do…”
Lasting effects on functioning among participants who found the SEM Glove useful in ADL
Lasting effects after using the SEM Glove were reported (MS, stroke) and manifested as perceived improved mobility and strength (MS, stroke) as well as improved grip (MS, stroke) and coordination (stroke). Lingering paraesthesia in the hand after use was expressed as a positive result (stroke) as well as decreased spasticity after use in addition to improved mobility and coordination in the fingers (MS).
“It has given me a great deal; it got my hand going again….as I couldn’t use it before”
Using the SEM Glove also improved the awareness of the hand (MS, stroke).
“…the grip has improved and, as I said, it’s like my brain has learned that I have a left hand.”
While others found no lasting effects on hand function (MS, stroke).
“It is just as flaccid and indifferent as before”
Level of functioning needed for beneficial effects of using the SEM Glove among participants who found the glove useful in ADL
Some participants stated that the SEM Glove should have been introduced earlier when the participant still had a higher level of functioning (MS).
“The positive side is that the glove helps the grip and on the negative side is that I should have had it earlier before my ability disappeared.”
Other participants found that the SEM Glove would be more suitable for people with a higher level of functioning and impairments related only to endurance (MS, stroke) or grip (MS), and who were able to open their hand fully voluntarily (stroke) or needed assistance only for the dominant hand (MS).
“Hold things during a longer period of time but… Yes, but I suppose I would recommend someone who thinks that´s their main problem… For me it’s more like I believe that my arm is too weak and I’m too weak outwards, to stretch my fingers.”
Learning period among participants who found the SEM Glove useful in ADL
The participants experienced a learning period, during which they learned how to individualize putting on the glove, and to get used to the SEM Glove in activities (MS, stroke). Experiences of finally using the glove spontaneously were reported, but also that some activities were avoided due to the shortcomings of the glove (stroke).
“It’s that thing about increasing the strength and those things with the fingertips and so on….and it took a while before I learned….for me, anyhow, it was complicated…Before you got used to the feeling of it, right.”
Activity performance related to the construction of the SEM Glove among participants who found the glove useful in ADL
The construction of the SEM Glove was found to support the wrist, which in turn supported the grip (stroke), while others found that the glove did not support the wrist (MS, stroke), which, e.g. limited the ability to write with a pen (stroke) and regretted that additional wrist support could not be combined with the glove (MS).
“…So it was both good and bad. In one way I could hold the pen better because then you use a three-finger grip… so it felt as it would have worked well if I had been able to move my wrist better… because that should also be included.”
In addition, the SEM Glove was found to trigger spasticity, and this made the thumb move in a movement trajectory where the sensor of the thumb did not connect to the object (MS), while others found it to be too slow for fast movements, e.g. when playing the guitar (stroke).
Moreover, the motor unit and cord were found to be too heavy and clumsy (MS, stroke) and restricted mobility, e.g. when changing from a standing to sitting position, going to the toilet or when kept in a bag on the wheelchair (MS, stroke). The glove, cord and motor unit were found to hinder putting on shirts, jackets and gloves and the glove could not be fitted under a winter glove or winter clothing (MS, stroke).
“I had imagined something more modern.. almost an invisible, small, slim, electronic gadget. So, it feels rather bulky and the cord is rather thick. The same goes for the computer that you are supposed to put somewhere.”
The plastic component in the palm of the hand was found to hinder the grip when handling objects (MS, stroke) and could negatively affect the motivation to use the SEM Glove (MS).
The fabric was found to affect sensory function negatively and was yet another reason for experienced limitation in writing while using the SEM Glove (stroke). The fact that the glove could not be used with an iPad® was perceived as negative, as the fingertips of the glove had to be lifted away temporarily (MS). Yet, fingers were also found to be supported by the fabric of the glove when writing on the computer (MS). As the participants had been informed that the glove was not water-resistant, use in activities involving water, such as hand-washing and other self-care activities, were found to be a restricting factor (MS, stroke). The fact that users had to wear a plastic glove on top of the glove for protection when cooking made it even more difficult to use (stroke).
“It is really hard that you can’t feel the pen.”
“But, on the negative side is that you can’t use it in water. If I’m to rinse something in the sink, I must….then it´s only the right arm I can use and I can’t wash my hands either. “
Donning and doffing was also found to be problematic (MS, stroke). One participant could not put on the SEM Glove without assistance and had to wear the glove between activities, although the participants would have preferred to take it off (MS). The fact that the batteries needed to be replaced and that the glove was difficult to put on made one participant use the glove less and less (MS).
“In the beginning it was problematic… because… my fingers are so stiff, you know…. and then it’s a bit…. you learn to open out all five fingers. It can be problematic.”
Another aspect experienced by participants in the positive group was the lack of assistance in opening the hand in order to initiate the grip and loosen the grip voluntarily (MS, stroke). This was reported to be due to the participants’ impaired extension function of the fingers (MS, stroke).
“Really my…I’m quite strong in clenching my hand, but I’m really weak when it comes to opening it.”
“But I feel that, for my complaints, it would have been better if I had put on the glove upside down… then you can let go.”
Body function and activity performance in ADL among participants who did not find the SEM Glove useful in ADL
None of the participants in this group identified ADL where the SEM Glove was perceived as being useful (MS, stroke). A shortcoming of the glove was reported as being related to its limitations in assisting in handling objects requiring fine hand use including involvement of the index finger (MS, stroke).
“Well, yes, it´s the fine hand use that’s my problem, but it was not of any use”
Again, the SEM Glove, cord and computer were found to be too bulky and heavy and too complicated to handle while dressing, moving, and transferring from a wheelchair, e.g. while using the toilet (MS, stroke). Another negative aspect experienced in this group was the lack of assistance with opening the hand in order to initiate the grip and loosen the grip voluntarily (MS).
“If you get assistance with the grip, in itself, that’s good but then if you need to get it back, like me, I have difficulties with my left hand to get it to open up, like this.”
Other participants found that although the grip around an object was tightened with assistance of the SEM Glove, the participant could still not perform the activity due to proximal weakness of the wrist or arm (MS)
“I can’t say that it was very positive, although there was a good grab around the glass because then I have difficulty lifting this arm towards my mouth.”
Lasting effects on functioning among participants who did not find the SEM Glove useful in ADL
The participants experienced no lasting effects on hand function (MS, stroke).
“No, the same as usual, the same as usual”
Activity performance related to the construction of the SEM Glove among participants who did not find the glove useful in ADL
Again, the SEM Glove, cord and motor unit was found to be too bulky and limiting movement and mobility (MS, stroke). The plastic component in the palm of the hand was another aspect that negatively affected the participants’ ability and motivation to use the glove (MS).
“As there is a hard device in the palm of my hand I can’t walk with my crutches and I walk with my crutches all the time, you know”
The SEM Glove was not found to be assistive, as the sensors were not found to touch smaller objects, such as a knife and fork, a plate, the handle of a jug, a cup or buttons (MS).
“If the sensors had touched the cutlery, but they sort of ended up on the side, or how to put it. You don’t hold the cutlery that way, really, right on the fingertips like this, but on the side, or how to put it.”
This explorative study demonstrates both the potential and limitations of the current version of the SEM Glove when used as an ADL assistive tool by people with impaired hand function due to prior stroke or MS. The weekly follow-ups and semi-structured interviews showed that participants tested the SEM Glove in a wide range of activities, indicating that expectations were high, although not always met. The interview results also reflect the complexity of everyday life use of the arm and hand where a single activity may involve not only grasp but also grip and pinch and complex fine hand use (33). Usability was clearly related to activities requiring a strong and prolonged grip, but not fine hand use, which might instead be negatively affected by the glove.
Overall, the results from the interviews showed that there were more participants who were positive about using the SEM Glove than those who were negative, and the perceptions of using the glove were shared both by participants with stroke and MS. Using a mixed methods embedded design, perceived usability in terms of a stronger grip was found among a group of participants with impaired grasp, grip and pinch, but who could achieve points around the mid-third of the ARAT total score and with no or a mild sensory impairment and independence in ADL. Participants who did not find the SEM Glove usable comprised both those with a high level of functioning, where the SEM Glove potentially hindered activity performance, such as fine hand use, but also participants, who could not participate in everyday ADL where the SEM Glove could be useful. Results from the current study could potentially be used as a guide in identifying people who may find the glove useful in the long-term. Still, not all participants fitted these descriptions and disadvantages were reported by all. Thus, expectations and intended use should be mapped thoroughly before recommending the SEM Glove.
Based on the results from the weekly telephone interviews, continued use over the 6 weeks’ intervention was found to decline in some participants, who did not find suitable activities due to overall disability. This agrees with observations from other studies. In a study of people living with mild to moderate impairments in the upper extremity in the long-term phase after stroke, perceived ability to perform hand ADL was associated not only with fine manual dexterity, including the ability to coordinate finger movements during grasping, manipulating and releasing the grip, but also with perceived participation in ADL (34). In a study of participants living with MS and moderate disability (mean Expanded Disability Status Scale (EDSS) 6), fine manual dexterity was also found to be associated with the ability to participate in ADL in the home setting (35). Together, these findings and previous reports suggest that to increase participation in daily life activities, an assistive glove must provide assistance in fine hand use.
The results from the interviews in the current study indicate that the SEM Glove may increase some wearers’ awareness of the hand, and potentially the use of the hand in ADL. Using assistive devices in the home setting may be a way to accomplish an activity level where the patient is more engaged in ADL, and that may induce an increase in level of functioning. It is worth noting that, among persons discharged home with a mean ARAT total score as high as 42 p, the daily activity level of the less-affected hand has been found to be 3 times higher than the affected hand at 12-months post-stroke, despite an increase to 57 p (max score) in mean (36). One plausible explanation is the so called “learned non-use”, meaning that the person compensates for their limitations in hand activities to a degree where they do not use the affected hand, e.g. because it is less strenuous and quicker to use the less-affected hand (37). Using an assistive glove could potentially increase the perceived usability of the hand in ADL, and thus prevent negative effects, such as “learned non-use”.
When using the SEM Glove and in future development projects in this area several factors need to be taken into consideration. Paresis of the hand due to CNS disorders is usually manifested by weakness, dyscoordination, disturbed spinal reflexes and muscle tone, as well as impaired sensory function. In case of severe paresis, abnormal hand posture due to spastic dystonia as well as co-contraction of antagonist muscles during voluntary activation may be seen, which offer significant challenges that always need to be considered for these patients. Furthermore, most often not only the hand is affected but the whole upper extremity is impaired as well as trunk and lower extremity function. Cognitive functions may also be affected, resulting in, for example, impaired attention, executive and memory functions, which may contribute to a limited activity level and participation (35, 38). During rehabilitation, this complexity of impairments and activity limitations must be considered when goals are set for regaining functioning at a level where the patient can return home with an activity level that enables maintained and/or further regained functioning.
In the current study, limitations related to the construction of the SEM Glove were pointed out by the participants in the interviews. These were related to placement of the sensors, the fabric and the speed of the movements and should be considered in the further development of the glove so as to increase its usability. Furthermore, the size, weight and placement of the cord and computer were issues reported to limit continuous use. The reported problems in putting on the glove indicate that the wearer needs to be able to relax and extend their fingers. These requirements are commonly not met among persons with CNS disorders, due to increased muscle tone and impaired motor function. Instead self-sufficiency is limited and an immediate access to assistance with donning and doffing is needed. This issue needs to be addressed, as a requirement for continuous use in ADL is that the wearer can put the glove on and take it off without too much time and effort. In a new version of the glove, called the Carbonhand (https://www.bioservo.com/healthcare), the ease of putting on the glove has been considered in the design.
A key limitation of the current version of the SEM Glove is the lack of an opening function. In the interviews, the need for assistance in opening the hand and fingers was commonly reported by the participants within a wide range of functioning and not only as a matter related to putting on the glove, but for a number of everyday life activities. The ability to actively extend the wrist and fingers is commonly impaired after a CNS lesion with upper extremity paresis (37, 39). Thus, to meet the needs of a vast population living with limited hand function due to CNS disorders, assistance in opening function is a crucial function in addition to the closing function of an assistive and/or rehabilitative robotic glove.
The need for wrist support is another issue that was clearly expressed in the interviews in this study. The ability to actively extend and sustain the extension of the wrist is crucial for producing a powerful grasp and grip and is often seen in impaired hand function due to injury or disease in the CNS (37, 40, 41). The current version of the SEM Glove does not provide support to the wrist, and not all participants were able to use their external wrist support with the SEM Glove. Further development of a glove should preferably include adjustments to enable the use of various wrist supports currently on the market, and the development of a dynamic wrist support is highly recommended in further development of the SEM glove.
The further development of assistive and training devices for persons with impaired hand function will probably also include other command systems than those used in the current version of the SEM Glove. Electromyography is already used in some exoskeletons, in refined prostheses for amputees, and in the development of a soft orthosis (42, 43), and brain-machine interfaces may open new opportunities.
Study limitations and strengths
This was a small explorative study performed at a single academic neurorehabilitation centre serving a single urban region. Thus, data do not allow general conclusions to be drawn. However, the study protocol was based on broad clinical experience in the area, on information from a preceding focus group (unpublished data) and study participants represented a wide range of typical impairments. The mixed methods design, providing consistent qualitative and quantitative data, support the observations and conclusions.
Conclusion
This explorative study provides information on expectations and perceived usability of an assistive glove, such as the SEM Glove, when used in the home setting by people living with paresis due to a CNS lesion. The SEM Glove was expected to be used in various activities, including grasp, grip and pinch movements. The results suggest that a majority of the participants, who found the SEM Glove to be useful in some ADL and/or improved in functioning, scored around the mid third on the total ARAT score and had a higher level of independence according to the BI.
This study highlights important aspects for consideration in the further development of new hand robotics. There is still a need for development of soft robotics gloves for rehabilitation and assistance in ADL due to CNS lesions that can assist in supporting the wrist and both opening and closing the hand and fingers. In the home setting, the glove should not hinder fine hand use and preferably should provide assistance with sufficient speed and accuracy to be considered fully usable by the wearer.
The authors would like to thank the participants who shared their valuable experiences and the data collector, reg physiotherapist Hanna Bergling
Conflicts of interest. SEM Gloves used by the participants in the study and financing were provided by Bioservo Technologies Inc. Representatives from Bioservo Technologies Inc. trained the therapist in the fitting and setting of the SEM Glove, but were not otherwise involved in methods, data collection, analyses or manuscript writing. Funding was also provided by a donation by Lars Hedlund (Karolinska Institutet Dnr 2-1582/2016). Researchers involved in the study have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize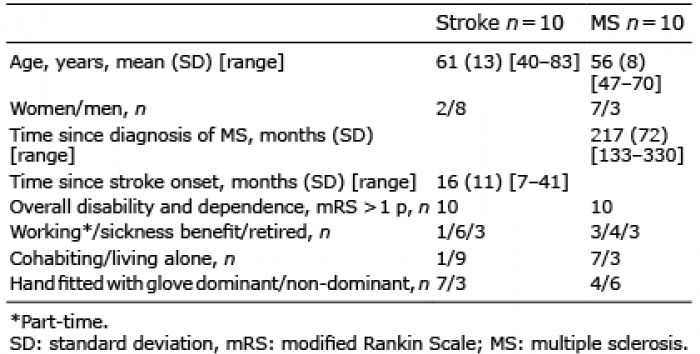 Click to show fullsize
Click to show fullsize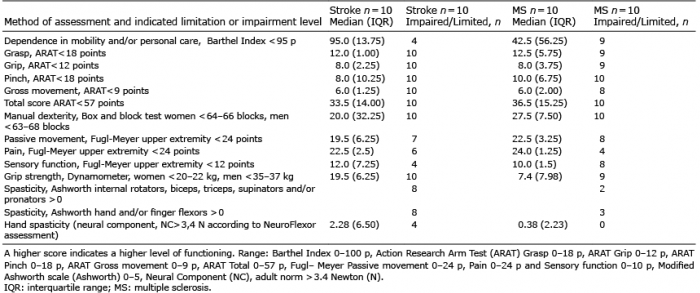 Click to show fullsize
Click to show fullsize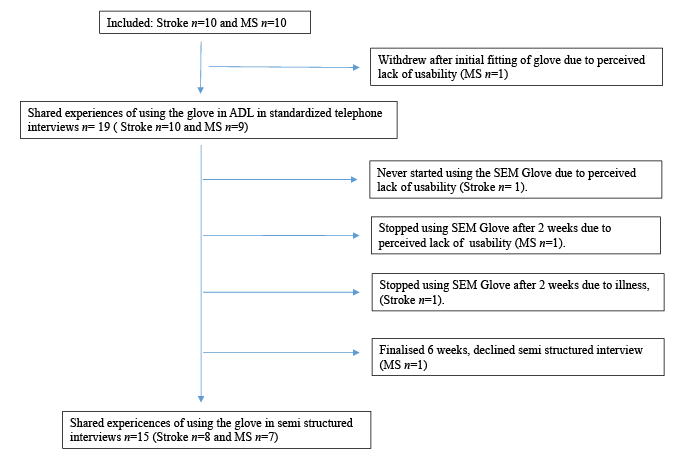 Click to show fullsize
Click to show fullsize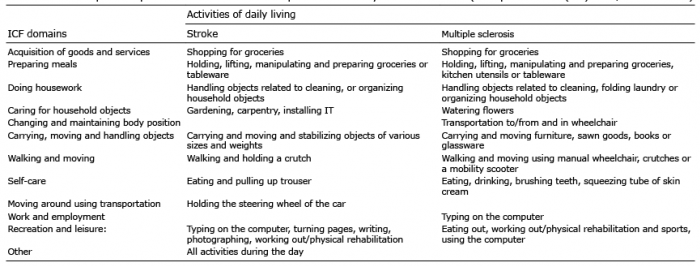 Click to show fullsize
Click to show fullsize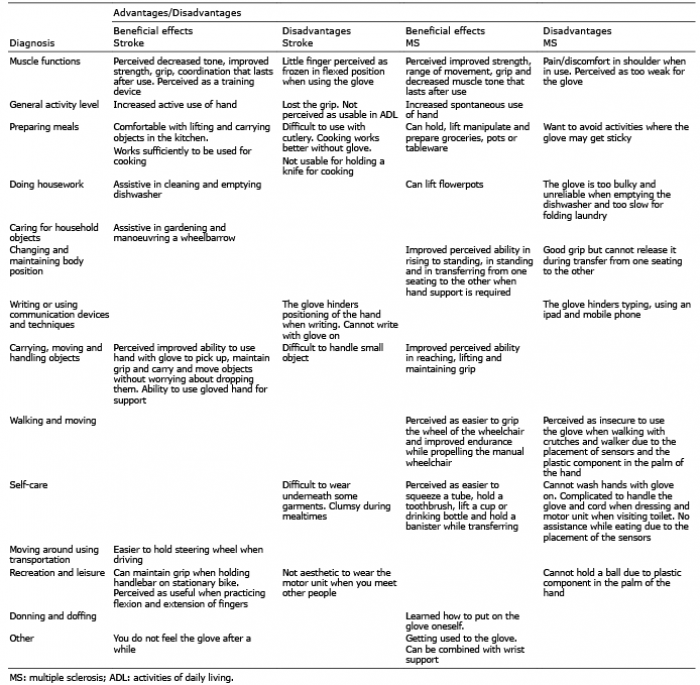 Click to show fullsize
Click to show fullsize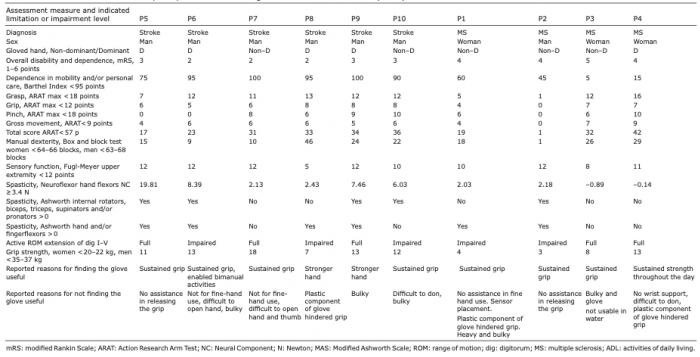 Click to show fullsize
Click to show fullsize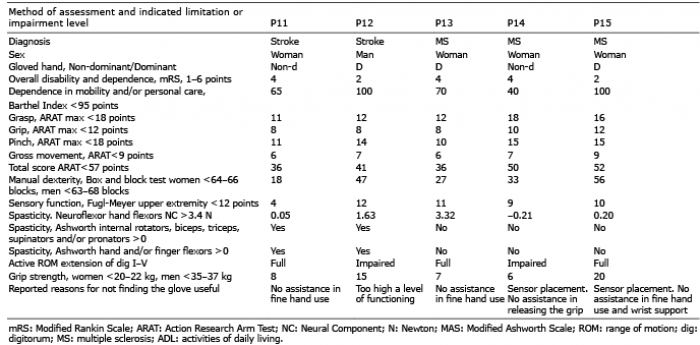 Click to show fullsize
Click to show fullsize